From Static Detailing to Video-First: Why Pharma Brands Are Making the Switch
Dushyant Sapre
May 26, 2026
There is a moment in most pharma brand planning cycles where someone pulls up the e-detailing usage report and the room goes quiet. Slide deck opens: high. Time per slide: 11 seconds. Completion rate: 23 percent. Repeat views: negligible. The materials were opened. They were not consumed.
This is the static detailing problem in numbers. And it is not getting better with more slides, better design, or shorter PDFs. It is a format problem. The format was built for a world where a doctor had five minutes, a printed brochure was the best available medium, and the MR could narrate the content live. None of those conditions reliably hold anymore.
Video-first detailing is not a trend. It is the logical response to how HCPs actually process information in 2026. And the pharma brands making the switch are not doing it because it is fashionable. They are doing it because the engagement data is impossible to argue with.
What Static Detailing Actually Costs
Before looking at why video works better, it is worth being precise about what static detailing is costing pharma brands in ways that do not show up on a single line item.
The first cost is attention. A 40-slide e-detailing module takes roughly eight to twelve minutes to read at a normal pace. Almost no doctor in a clinical setting has eight to twelve uninterrupted minutes to devote to a pharma brand communication. The module gets opened, skimmed, and closed. The MR reports it as a completed detail. The brand team counts it as an engagement. Nothing actually changed in the doctor's clinical thinking.
The second cost is recency. Static materials take weeks to produce and approve. By the time a new clinical study or competitive development is incorporated into the approved detailing material, the moment when that information would have been most valuable has often passed. Brand teams that cannot respond quickly to the clinical conversation happening right now are ceding ground to whoever can.
The third cost is differentiation. When every company in a therapy area is delivering information through similar e-detailing formats, the format itself creates no advantage. The information has to work harder to break through. Video creates a perceptual break from the standard detailing experience, which is part of why completion rates are consistently higher.
Why Video Works for HCP Communication
The evidence base for video as a more effective HCP communication format is now substantial enough that the question is not really whether it works. The question is how to deploy it within the specific constraints of pharma promotional communication.
The core cognitive argument is that video combines visual and auditory processing in a way that text-based materials cannot match. Information presented in a well-structured 90-second video is retained more effectively than the same information presented as a slide or PDF. For complex mechanisms of action, comparative efficacy data, or safety profiles, the format advantage is particularly pronounced.
The practical argument is that video fits the consumption context of a busy HCP in a way that slides do not. A two-minute video can be watched during a break, between patients, or during a commute. It does not require the focused, screen-centred attention that reading a detailed slide deck demands. This means more of the content actually gets consumed, not just opened.
The engagement argument is that completion rates, replay rates, and share rates for short-form pharma video consistently outperform equivalent metrics for static materials. When a doctor replays the mechanism of action segment of a reel, you have a clear signal about their interest level that no slide deck engagement metric can match.
The Practical Barrier That AI Has Just Removed
Every pharma brand manager who has looked seriously at video-first detailing has run into the same wall. The cost and timeline of video production made it practical only for major product launches or high-priority molecules. Everything else continued to be serviced by static materials because there was no viable alternative at the required scale and cost.
AI video generation has removed that wall. Tools like MagicReel, part of SwishX's Marketing IQ platform, convert a product monograph or approved promotional document into a 60 to 120 second branded video reel in approximately 8 to 12 minutes. The output includes visuals, voiceover, and a script structure optimised for the target audience, whether that is a specialist HCP, a general practitioner, or an MR. The cost per reel is a fraction of traditional production, making it economically viable to produce video content for every molecule in the portfolio, not just the marquee brands.
This changes the feasibility calculation entirely. A brand team that was previously choosing between video for two products or static for ten can now have video for all ten. And because the content is generated from approved source documents, the compliance starting point is solid rather than speculative.
For a detailed breakdown of what AI video production costs and what the compliance workflow involves, read our piece on AI-generated doctor videos for pharma.
How the Switch Actually Happens
The transition from static to video-first detailing does not have to happen all at once. The most common and most successful approach is to start with the therapy areas or molecules where HCP engagement is most critical and where the current static materials are performing worst.
For each priority product, the process involves converting the approved promotional content into video format, running it through the existing medical-legal approval workflow, and deploying it through the same distribution channels currently used for static materials: primarily WhatsApp, email, and the MR detailing tool.
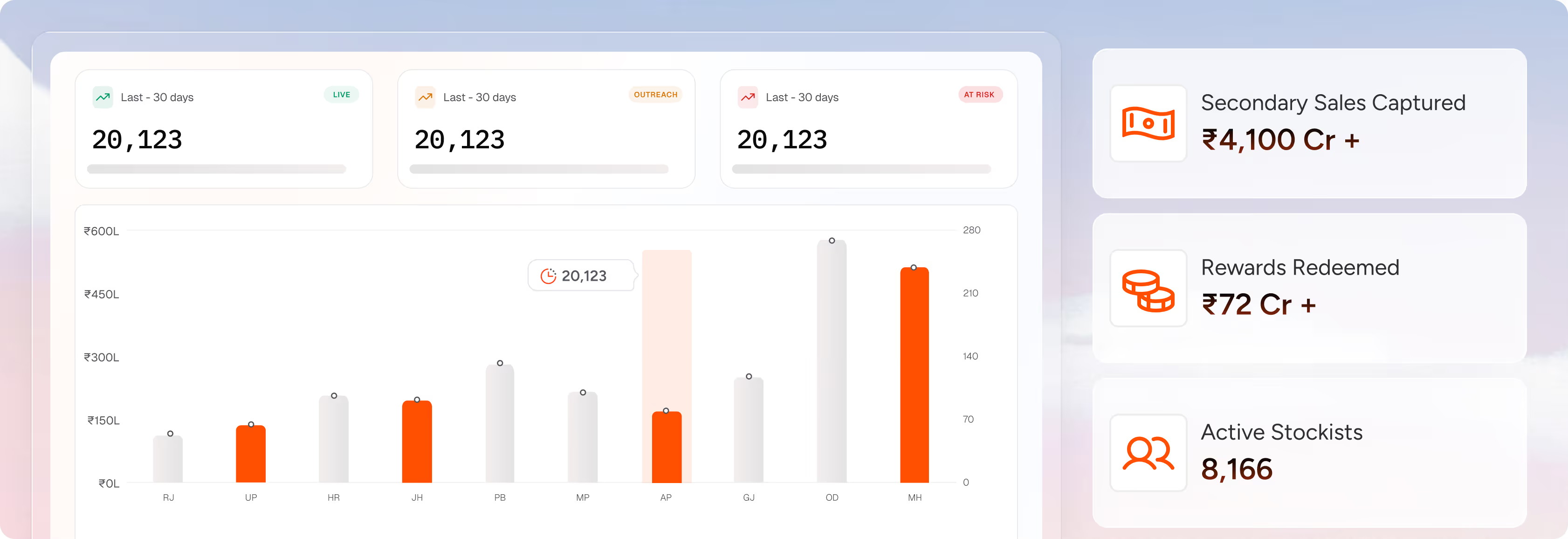
The first cycle typically produces a measurable engagement uplift that becomes the internal business case for broader rollout. Video completion rates, replay patterns, and share behaviour are visible in the platform analytics by HCP segment, geography, and therapy area. The data that comes back from the first deployment tends to accelerate the case for the second.
The MR workflow integration is worth addressing specifically because it is where many video-first transitions stall. MRs who have been trained on slide-based detailing often need support adapting to a video-first call structure. The practical reality is that showing a 90-second reel and then facilitating a conversation around it is a more effective use of limited face time than walking through slides. But this requires training and a period of adjustment. Companies that invest in this transition alongside the content format change see faster adoption and better commercial outcomes.
What the Data Looks Like After the Switch
The engagement metrics that come back from video-first detailing programmes are consistently more useful than what static materials produce. Not just because the numbers are better, though they generally are, but because the signal is richer.
Slide deck analytics tell you that a deck was opened. They do not tell you which slides held attention, which were skipped, or which prompted the doctor to call the MR with a question. Video analytics tell you exactly where in a reel attention peaked, where it dropped, which segments were replayed, and which HCP profiles showed the highest completion rates. This is the kind of data that actually helps a brand team improve the next piece of content rather than just report that the last one was distributed.
For pharma brand managers who want to understand how HCP field force activity data connects to downstream commercial outcomes more broadly, our piece on activity versus impact covers that measurement gap in detail.
The Competitive Case for Moving Now
The shift from static to video-first detailing is not happening uniformly across the Indian pharma industry. Some companies are already operating with video-first content libraries for their top therapy areas. Most are still debating it. A few are waiting to see what competitors do.
The companies in the first group are building something that the others are not: a content engagement data set that gets richer with every deployment cycle. They know which video formats work for cardiologists in tier 1 cities. They know how long the attention window is for a diabetologist watching a mechanism of action reel. They know which opening frames drive completion and which lose the viewer in the first 10 seconds. This knowledge is not transferable. It has to be earned through deployment, and the earning takes time.
Waiting for the transition to become industry standard before making it is a strategy that guarantees arriving late to a compounding advantage.
Static e-detailing modules are opening but not being consumed. Average slide view times have compressed to seconds, and completion rates for long-form PDF materials are in the low double digits. Video drives meaningfully higher engagement because it fits the consumption context of a busy HCP and is retained more effectively than text-based content.
With AI tools like MagicReel, the content generation step takes approximately 8 to 12 minutes from document upload to finished reel. The total cycle time including compliance review depends on your internal approval workflow, but the production bottleneck has been effectively eliminated.
WhatsApp is the dominant distribution channel for pharma video content reaching HCPs in India, with the highest open and completion rates across most specialty segments. Email is a secondary channel for certain HCP profiles and institutional contacts. Rep-assisted distribution during or after a detail visit is increasingly common as MRs shift to video-first call structures.
Video content distributed to HCPs is subject to the same UCPMP requirements as any other promotional material. Compliance depends on ensuring all claims are sourced from approved prescribing information, off-label content is excluded, and the material is directed only at qualified healthcare professionals. AI tools that generate content from approved source documents provide a stronger compliance starting point than traditional production workflows.
.avif)














.svg.avif)